1-Normally, when you put the patient on the bed, the neck of the femur is raised above surface of the table, the angle between the table and femur neck is known as femoral neck anteversion angle.
2-For CT evaluation, put the patient supine with both lower limbs symmetrically in the same position.
3-Then, take sections in hip and knee.
4-Choose the section where the patella is largest and well defined, and the section where it passes through neck of the femur.
5-Draw a line in the middle of the femoral condyle and in the middle of the femoral neck.
6-Calculate the angle between these two lines.
7-Normal values of the angle in respect to the age of the patient:
-0-1 y = 30-50.
-2 y = 30.
-3-5 y = 25.
-6-12 y = 20.
-12-15 y = 17.
-16-20 y = 11.
-20 y = 8.
The femoral neck anteversion angle is an important factor for hip
stability and normal walking.
It is multifactoral result of evolution,
heredity, fetal development, intrauterine position, and mechanical
forces.
Abnormal FNA sometimes can be associated with many clinical
problems ranging from harmless intoeing gait in the early childhood, to
disabling osteoarthritis of the hip and the knee in the adults.
In most
cases is associated with minor functional problems in children during
growth, but cause a concern in parents for children future.
The child
must be examined carefully and an accurate diagnosis must be
established.
The most important part of care is observation of the
children.
If abnormal femoral neck anteversion produces severe
functional disability, derotational osteotomy should be done, but
delayed until late childhood.
 1, Ulna. 2, Radial head. 3, Lateral epicondyle. 4, Extensor carpi radialis longus muscle. 5, Olecranon fossa. 6, Medial epicondyle. 6a, Common flexor tendon. 7, Triceps muscle (lateral head). 8, Humerus. 9, Triceps muscle (Medial head). 10, Flexor digitorum superficialis muscle. 11, Supinator muscle. 12, Extensor digitorum muscle.
1, Ulna. 2, Radial head. 3, Lateral epicondyle. 4, Extensor carpi radialis longus muscle. 5, Olecranon fossa. 6, Medial epicondyle. 6a, Common flexor tendon. 7, Triceps muscle (lateral head). 8, Humerus. 9, Triceps muscle (Medial head). 10, Flexor digitorum superficialis muscle. 11, Supinator muscle. 12, Extensor digitorum muscle.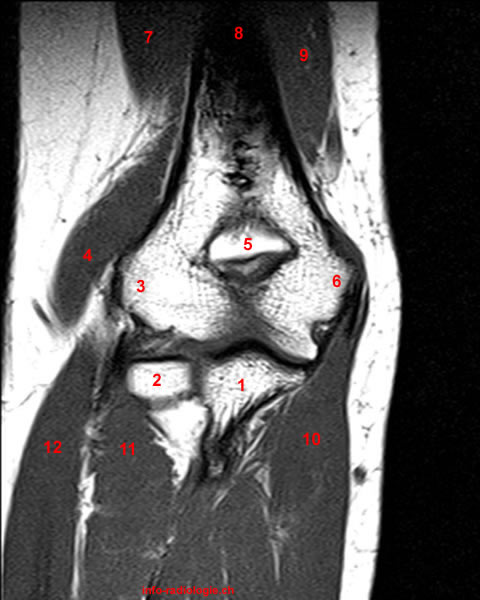










































{kind=link}