Peroneal tendon lesions.
Figure 1. Drawing illustrates the lateral ankle. The peroneus brevis (PB) and peroneus longus (PL)tendons descend posterior to the lateral malleolus and are held in place by the superior peroneal retinaculum (SPR) and inferior peroneal retinaculum (IPR). F = fibula. (Courtesy of Salvador Beltran, MD, Albons, Girona, Spain.)
Figure 2a. Axial (a) and sagittal (b) T1-weighted MR images demonstrate normal peroneus brevis (short arrow) and peroneus longus (long arrow) tendons descending posterior to the lateral malleolus (F). The peroneus brevis tendon is mildly crescentic in configuration on the axial image.
Figure 2a. Axial (a) and sagittal (b) T1-weighted MR images demonstrate normal peroneus brevis (short arrow) and peroneus longus (long arrow) tendons descending posterior to the lateral malleolus (F). The peroneus brevis tendon is mildly crescentic in configuration on the axial image.
Figure 2a. Axial (a) and sagittal (b) T1-weighted MR images demonstrate normal peroneus brevis (short arrow) and peroneus longus (long arrow) tendons descending posterior to the lateral malleolus (F). The peroneus brevis tendon is mildly crescentic in configuration on the axial image.
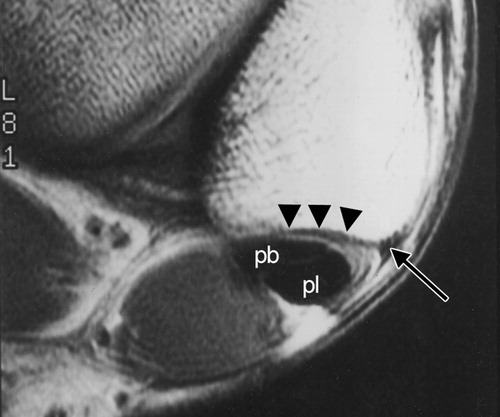
Figure 4. Axial T1-weighted MR image depicts a normal concave retromalleolar groove (arrowheads). A fibrous ridge is noted at the origin of the SPR (arrow). pb = peroneus brevis tendon,pl = peroneus longus tendon.
Figure 5. Axial T1-weighted MR image depicts an irregular retromalleolar groove (arrowheads), which predisposes to peroneal tendon disease.
Figure 6. Medial pseudosubluxation of the peroneus brevis tendon. Axial T1-weighted MR image demonstrates the peroneus brevis tendon (short arrow) medial to the tip of the fibula simulating a subluxation. Long arrow indicates the peroneus longus tendon.
Figure 7. Axial T1-weighted MR image shows a normal peroneal tubercle (large*) and retrotrochlear eminence (small *). The peroneal tubercle separates the peroneal brevis (short arrow) and peroneus longus (long arrow) tendons.
Figure 8a. Hypertrophic peroneal tubercle. Axial (a) and coronal (b) T1-weighted MR images depict a bone protuberance (*) between the peroneus brevis (short arrow) and peroneus longus (long arrow) tendons.
Figure 8b. Hypertrophic peroneal tubercle. Axial (a) and coronal (b) T1-weighted MR images depict a bone protuberance (*) between the peroneus brevis (short arrow) and peroneus longus (long arrow) tendons.
Figure 9. Axial T1-weighted MR image depicts a hypertrophic retrotrochlear eminence (*). A peroneus quartus tendon, which is commonly associated with hypertrophy of the retrotrochlear eminence, is also identified (arrow).
Figure 10. Drawing illustrates a peroneus quartus muscle (arrowheads) located posterior to the peroneus brevis (long straight arrow) and peroneus longus (short straight arrow) tendons. Its most common insertion site is the retrotrochlear eminence of the calcaneus (curved arrow). (Courtesy of Salvador Beltran, MD, Albons, Girona, Spain.)
Figure 12. Axial T1-weighted MR image shows direct insertion of a peroneus quartus muscle (m) onto the calcaneus (C).
Figure 13. Peroneus quartus tendon simulating a torn peroneus brevis tendon. Axial T1-weighted MR image demonstrates a peroneus quartus tendon (long arrow) in proximity to the peroneus brevis tendon (short arrow). This finding should not be mistaken for a peroneus brevis tendon tear.
Figure 16. Peroneal tenosynovitis. Axial T2-weighted MR image shows a large amount of fluid (*) within the common peroneal tendon sheath with preserved tendon morphologic features.
Figure 17. Axial T1-weighted MR image demonstrates the calcaneofibular ligament (arrowheads) in proximity to the peroneal tendons (arrow). Tear of the calcaneofibular ligament can cause fluid accumulation in the peroneal tendon sheath and simulate tenosynovitis.
Figure 18. Stenosing tenosynovitis following ankle ligamentous repair. Axial T1-weighted MR image demonstrates abundant low-signal-intensity scar tissue lateral to the calcaneus (arrows). The tendons cannot be distinguished from the scar tissue.
Figure 20a. Longitudinal tears of the peroneus brevis tendon. (a) Axial T1-weighted MR image depicts a fragmented peroneus brevis tendon (short straight arrows) with an advanced tear and a markedly thinned central portion (curved arrow). Long straight arrow indicates the peroneus longus tendon. (b) Axial T1-weighted MR image obtained in a different patient shows a split of the peroneus brevis tendon (short arrows) and anterior migration of the peroneus longus tendon (long arrow).
Figure 20a. Longitudinal tears of the peroneus brevis tendon. (a) Axial T1-weighted MR image depicts a fragmented peroneus brevis tendon (short straight arrows) with an advanced tear and a markedly thinned central portion (curved arrow). Long straight arrow indicates the peroneus longus tendon. (b) Axial T1-weighted MR image obtained in a different patient shows a split of the peroneus brevis tendon (short arrows) and anterior migration of the peroneus longus tendon (long arrow).
Figure 21. Concomitant peroneus brevis and peroneus longus tendon tears. Axial T1-weighted MR image depicts increased intrasubstance signal intensity in both the peroneus brevis (short arrow) and peroneus longus (long arrow) tendons.
Figure 23a. (a) Complete peroneus longus tendon tear. Oblique coronal T2-weighted MR image shows absence of the peroneus longus tendon (arrows) underneath the cuboid bone (*). (b) Oblique coronal T2-weighted MR image obtained in a different patient shows a normal peroneus longus tendon (arrow). * = cuboid bone.
Figure 23b. (a) Complete peroneus longus tendon tear. Oblique coronal T2-weighted MR image shows absence of the peroneus longus tendon (arrows) underneath the cuboid bone (*). (b) Oblique coronal T2-weighted MR image obtained in a different patient shows a normal peroneus longus tendon (arrow). * = cuboid bone.
Figure 24a. (a, b) Complete peroneus longus tendon tear associated with cuboid bone marrow edema. (a) Sagittal fat-suppressed T2-weighted MR image demonstrates a thickened and retracted peroneus longus tendon (arrows). F = fibula. (b) Adjacent section from the same MR imaging study depicts high-signal-intensity bone marrow edema in the cuboid bone (white arrows). The peroneus longus tendon (black arrow) is not visualized in the cuboid tunnel. (c) Sagittal MR image obtained in a different patient shows a normal peroneus longus tendon (arrow) underneath the cuboid bone (*).

Figure 27. Drawings illustrate Oden’s surgical classification system for SPR injuries. A normal SPR originates from the distal fibula (A). A small fibrous ridge may be found at the attachment site. In type I injury (B), the SPR is stripped off the distal fibula, forming a pouch into which the peroneal tendons can dislocate. Type II injury (C) is a tear of the SPR at its attachment to the distal fibula. Type III injury(D) is an avulsion fracture of the SPR at its attachment to the distal fibula. Type IV injury (E) is a tear of the SPR at its posterior attachment. PB = peroneus brevis tendon, PL = peroneus longus tendon. (Reprinted, with permission, from reference 21.)
Figure 28. Axial T1-weighted MR image shows a normal low-signal-intensity SPR (thick straight arrows) holding the peroneal tendons (curved arrow) within the retromalleolar groove. Thin straight arrow indicates the fibrous ridge at the fibular attachment site of the SPR. (Reprinted, with permission, from reference 21.)
Figure 29. Type I SPR injury. Axial spin-echo proton-density–weighted MR image demonstrates dislocation of the peroneal tendons (thick white arrow) into the pouch formed by a stripped-off SPR and periosteum (thin white arrows). The fibular groove (black arrow) is slightly convex. Degenerative changes at the posterior subtalar joint are incidentally noted. (Reprinted, with permission, from reference 21.)
Figure 30. Type I SPR injury with a collapsed pouch in a patient with clinical recurrent peroneal tendon dislocation. Axial T1-weighted MR image shows a linear area of low signal intensity (short arrows) lateral to the distal fibula (F), a finding that is consistent with a collapsed pouch. The peroneal tendons (long arrow) are in their normal position. (Reprinted, with permission, from reference 21.)
Figure 31. Type II SPR injury. Axial T1-weighted MR image depicts a tear close to the fibular attachment of the SPR (black arrow). The peroneal tendons (white arrow) are dislocated laterally. The fibular groove (arrowhead) is flat.
Figure 33. Type III SPR injury. Axial fast spin-echo T2-weighted MR image depicts a torn and slightly retracted SPR (arrowheads). A cortical defect (straight arrow) and bone marrow edema (white *) are noted at the distal fibula. The peroneal tendons (curved arrow) are in their normal position within a convex fibular groove, but thinning and irregularity of the peroneal brevis tendon suggest impending longitudinal splits. Fluid is seen in the common peroneal tendon sheath (black *). (Reprinted, with permission, from reference 21.)
Reference




























No comments:
Post a Comment